Problems Associated with Inactivity
While PA has been shown to be beneficial to people of all ages, backgrounds, and abilities, there remains a general lack of engagement from a societal standpoint. Over the past 20 years obesity rates have continued to climb. Currently, about 1/3rd of all U.S. adults are obese while about 1/6th of U.S. children (12-19-year-olds) are considered obese. The Center for Disease Control (CDC) classifies individuals having a Body Mass Index (BMI) greater than or equal to 30 as obese. An individual’s BMI examines the relationship between their height and weight and “can” be an indicator of body fatness, thus BMI serves as a potential screening tool but not necessarily as an assessment for body fatness.
CDC’s Overweight-Obesity Categories
| BMI Value | Classification |
| Less than 18.5 | Under Weight |
| 18.5 to 24.9 | Normal Weight |
| 25 to 29.9 | Overweight |
| 30 to 34.9 | Obese Class I |
| 35 to 39.9 | Obese Class II |
| 40+ | Obese Class III (severe) |
Even more troubling than the percentage of Americans considered obese is the established relationship between obesity and many chronic disease states such as diabetes, heart disease, and cancer. The data would suggest we seem to be headed in the wrong direction. Additionally, complications resulting from many chronic disease states often include (but are not limited to) reduced quality of life and substantial financial hardship.
According to the CDC, obese folks, when compared to their normal or healthy weight counterparts, are at an increased risk for:
- All causes of mortality
- High blood pressure (hypertension)
- Higher levels of HDL cholesterol, lower levels of LDL cholesterol
- Higher levels of triglycerides (dyslipidemia)
- Type 2 Diabetes
- Coronary heart disease
- Stroke
- Gallbladder disease
- Osteoarthritis
- Sleep apnea
- Various cancers
- Lower quality of life
- Mental illness such as depression and/or anxiety
- Pain with physical function
It is not all doom and gloom however, as we will examine. While the mechanisms of obesity are multifactorial and complex, physical activity (PA) has been shown to have a tremendously positive impact on the prevention and treatment of obesity.

Exercise is Medicine
Like obesity, PA also has a relationship with many chronic disease states. Chiefly, PA helps prevent their development. PA has been shown useful in the prevention of the big three: heart disease, cancer, and stroke and the benefits don’t end there. In their Evidence Report, the National Institutes of Health (NIH) recommend PA as a leading strategy in the treatment of obesity, second only to dietary therapies.
Regular PA has also been shown to:
- Improve weight management efforts
- Increase force production (strength)
- Reduce body fat
- Promote bone, muscle, and joint development
- Improve heart and lung function / capacity
- Improve endurance
- Improve sleep quality
- Decrease depression risk
- Improve energy and self esteem
- Decrease stress
- Increase life expectancy
Let us now narrow our scope and focus specifically on the benefits of resistance training.
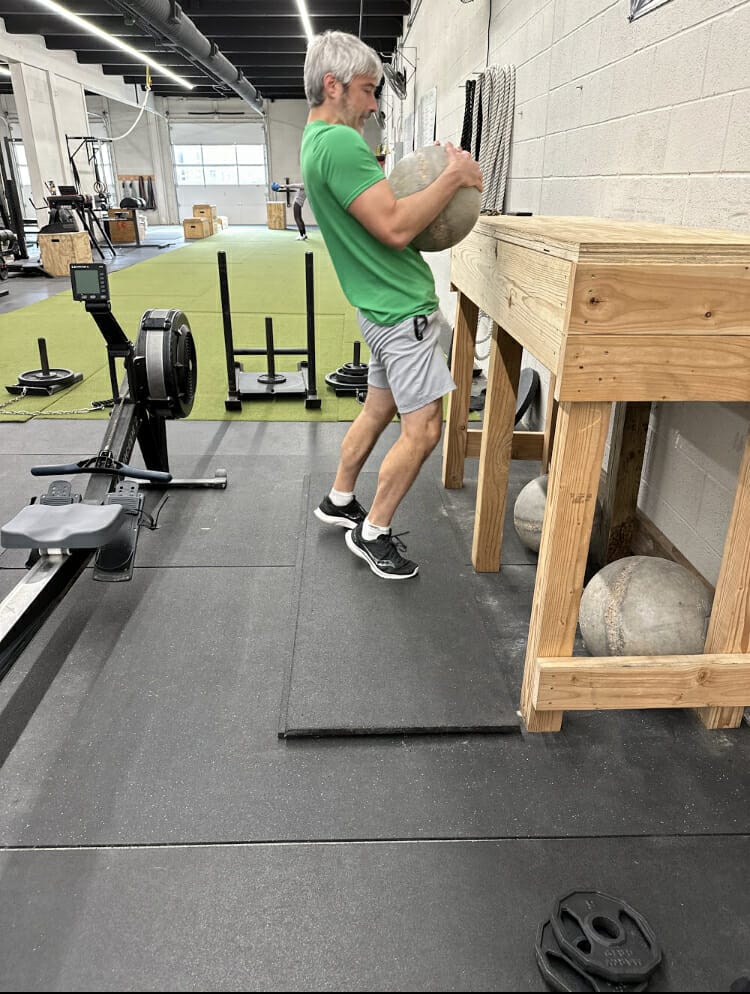
Benefits of Resistance Training
In order to understand the benefits of resistance training, some definitions are likely in order. We will define strengthas the ability to exert force against an external resistance. Therefore, resistance training is physical activity that is designed to increase force production (i.e. strength).
Below is a list of Jim Cawley’s 10 physical traits that were expanded upon by CrossFit. While CF’s founder Greg Glassman notes “fitness” is correlated to one’s ability in each of the ten physical traits.
- Cardiorespiratory Endurance
- Stamina
- Flexibility
- Power
- Speed
- Coordination
- Agility
- Balance
- Accuracy
- Strength
Due to the often observed, carry-over impact seen with regular strength training, would make a case that strength has a unique “foundational” quality. When one increases his/her strength via resistance training, everything else gets a little better. This relationship is not seen, however, in reverse making strength a very desirable quality. For example, an athlete may get stronger and notice his mile time has dropped a bit (likely due to the increased force production capacity of the relevant musculature), however, the same athlete may be disappointed to find that while his mile time has dropped (via aerobic training), his 5 rep max deadlift has actually decreased in the absence of resistance training (likely due to insufficient mechanical stimulation of the relevant musculature).
While there is plenty of evidence to support the inclusion of aerobic training into one’s program, it becomes increasingly more difficult to justify significant time expenditure on other qualities such as balance, agility, accuracy, coordination, and flexibility. Our position is that it is in the best interest of the athlete (and coach) to focus on strength and aerobic development to most efficiently address all physical qualities of the athlete. Other qualities would only be addressed specifically if time and budget were not a concern.
Taking a more health-centered view, resistance training has also been shown very effective in the preservation of basic physical function (i.e., successfully navigating your environment), the prevention of osteoporosis (loss of bone mass), sarcopenia (loss of muscle mass), and low back pain due to the profound effects it has on the musculoskeletal system (more on pain later).

We hope this section effectively lays out our rationale for prioritizing resistance training in the programs of our athletes. To be clear, we are not suggesting that folks should prioritize resistance training at the exclusion of all other training interests … we simply see the promotion of resistance training in their programs as physically, professionally, and financially prudent.
Resources
- Center for Disease Control. Overweight and Obesity: https://www.cdc.gov/obesity/adult/defining.html
- Center for Disease Control. Overweight and Obesity. Causes and Consequences: https://www.cdc.gov/obesity/adult/causes.html
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. The Evidence Report. National Institutes of Health: https://www.nhlbi.nih.gov/files/docs/guidelines/ob_gdlns.pdfps://en.wikipedia.org/wiki/Hans_Selyeerliftingtowin.com
- https://www.verywellfit.com/how-many-walking-steps-are-in-a-mile-3435916
- Potential Health-Related Benefits of Resistance Training. RA Winett, RN Carpinelli – Preventive medicine, 2001 – Elsevier: https://www.sciencedirect.com/science/article/pii/S0091743501909090
- Rhodes, R.E., Martin, A.D., Taunton, J.E. et al. Factors Associated with Exercise Adherence Among Older Adults. Sports Med 28, 397–411 (1999). https://doi.org/10.2165/00007256-199928060-00003